|
|
Lung Abscess
General Considerations
- Cavitary lung lesions produced by infectious agents
- They may be consequences of aspiration (most commonly) or pneumonia or they may be secondary to bronchial obstruction, bronchiectasis, bacterial endocarditis or spread of infection from elsewhere in the lung
- Most abscesses are caused by mouth anaerobes in patients with pre-existing periodontal disease
- Alcoholics (most commonly), those with seizure disorders leading to aspiration and those with poor dentition are at a higher risk
- Anaerobes are most frequent cause; most lung abscesses are polymicrobial in etiology
- Bacteroides
- Fusobacterium
- Also
- Staphylococcus
- Streptococcus pyogenes
- Klebsiella
- Haemophilus influenzae
- Actinomyces species
- And, rarely
- Cryptococcus
- Histoplasma
- Blastomyces
- Coccidioides
- Mycobacterium
Clinical Findings
- Typically take 7-14 days from pneumonia to abscess formation, depending on agent
- Fever
- Cough
- Foul-smelling sputum production
- Hemoptysis
- Night sweats
- Anorexia and weight loss
Imaging Findings
- On conventional radiography

- Cavities typically have a
- Thick-wall (which may become thinner as the surrounding inflammation resolves)
- Smooth inner margin
- Air-fluid level
- More frequent in superior segments of lower lobes or posterior segments of lower lobes
- Unlike pleural collections, lung abscesses frequently have a fluid level which is approximately the same length on both the frontal and lateral projection
- About 1/3 may have an associated empyema
- Helpful in differentiating between a lung abscess and an empyema
- Cavity may be seen as rounded with a thick wall and an air-fluid level
- Lung abscesses, being intraparenchymal, form an acute angle where they meet the chest wall
Differential Diagnosis
Treatment
- Antibiotics for 4-6 weeks or until the chest radiograph shows resolution
- Percutaneous catheter drainage
- Surgery, either a lobectomy or pneumonectomy, may be used for patients who fail to respond to medical therapy
Complications
Prognosis
- With proper antibiotic treatment, over 90% are cured
- Those who are immunocompromised or have a bronchial obstruction have a high mortality rate

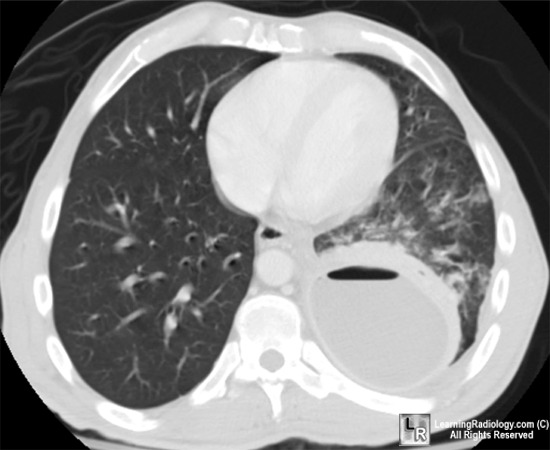
Lung abscess. A single, contrast-enhanced axial CT scan image of the chest shows a large cavitary lesion in the left lower lobe with a relatively thick wall(black arrows). The cavity has a smooth inner margin and an air-fluid level (white arrow). There is inflammatory reaction in the surrounding lung (yellow arrow). Notice the acute angle the abscess makes with the posterior chest wall.
For this photo without the annotations, click here
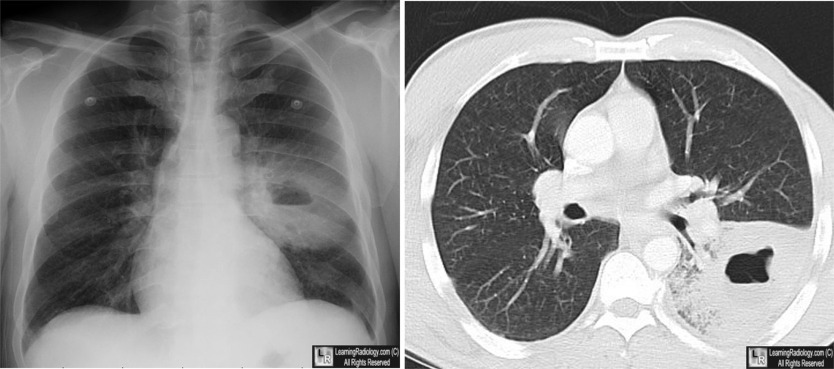
Lung Abscess. There is a thick-walled cavity with a smooth inner margin, located in the left lower lobe. An air-fluid level is present.
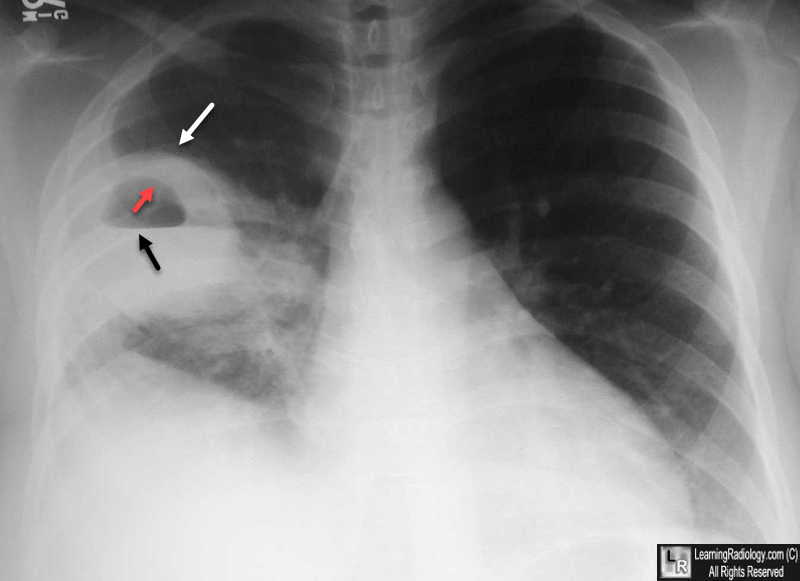
Lung Abscess. There is a thick-walled cavity with a smooth inner margin (red and white arrows). An air-fluid level is present (black arrow).
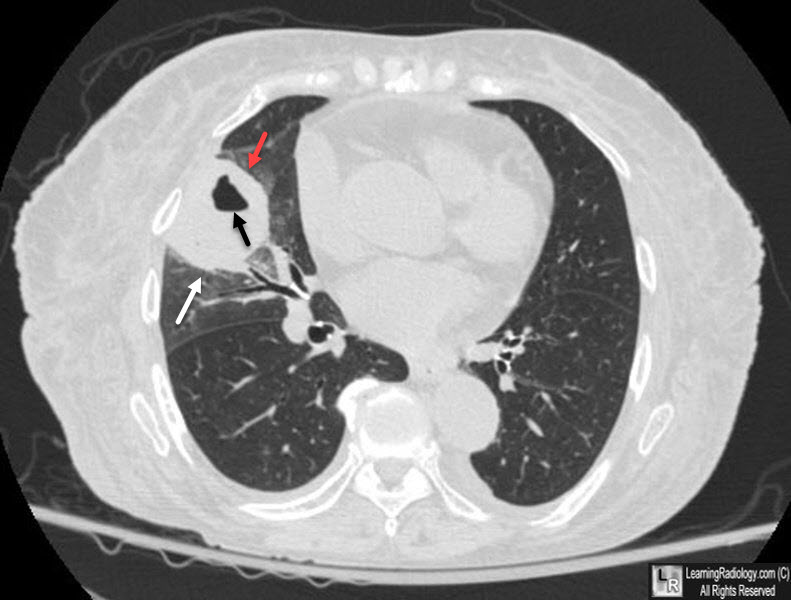
Lung Abscess. There is a thick-walled cavity (white arrow) with a smooth inner margin (red arrow), located in the right lung.
An air-fluid level is present (black arrow).
For more information, click on the hyperlinks indicated by this icon:
Lung abscess eMedicine Sharma, S. MD, FRCPC
|
|
|

){kind=link}
{kind=link}