|
|
Cephalohematoma
General Considerations
- Usually develops after delivery using instruments
- Subperiosteal hematoma
- No associated skull fracture
- Limited by suture lines
- Large cephalohematomas may occur with vitamin K deficiency in the newborn
Clinical Findings
- Soft tissue mass on head following instrument delivery
- Usually in the parietal region
- May not be visible at birth but should appear by day 2-3
Imaging Findings
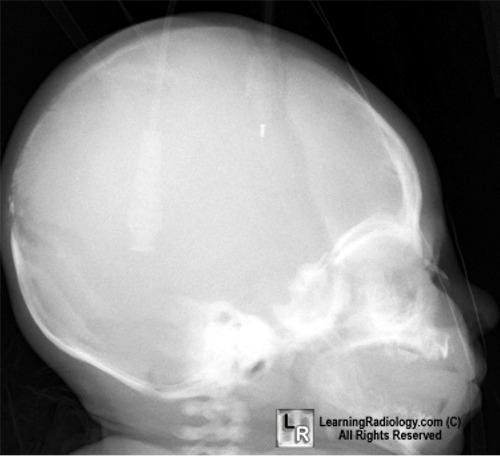
- Visible on conventional radiography as soft tissue subperiosteal elevation
- Usually over parietal bones, then occipital, and lastly frontal
- Sharply demarcated soft tissue density
- Outer border may calcify as a rim
- The skull may appear thickened at the site of the hematoma for years
Differential Diagnosis
- Subgaleal hemorrhage
- Into the subaponeurotic space from rupture of the emissary veins
- Crosses suture lines
- Covers a much larger area than a cephalohematoma
- Potentially life-threatening
- 50% occur with vacuum extraction
- Caput succedaneum
- Occurs after vaginal delivery
- Subcutaneous hemorrhage requiring no intervention
- Not limited by suture lines
Treatment
Complications
- Complications are rare
- Hyperbilirubinemia, if the collection is large
- Infection
- Calcification of the hematoma
Prognosis
- May take several months for complete resorption
 
Cephalohematoma. On the frontal skull radiograph on the left, these is a soft tissue mass (white arrow) in the soft tissues of the scalp. Notice how the mass does not cross beyond the sagittal suture line (black arrow). The lateral view shows the soft tissue mass is located in the parietal region (white arrow).
For additional information about this disease, click on this icon if seen above.
For same photos without annotations, click here or here
Williams Obstetrics 22nd Ed McGraw Hill
|
|
|

{kind=link}
{kind=link}