|
|
Difficult Endotracheal Intubation - Aspirated Tooth
General Considerations
- With difficult intubation, practitioner tends to increase lifting forces of laryngoscope blade
- May lead to damage of intraoral tissues and osseous structures
- Dental injuries associated with intubation
- Maxillary central incisors are at most risk
- Fifty percent of dental trauma from intubation happens during laryngoscopy itself
- 23% occurs following extubation
- Dental injuries are more common in
- Small children
- Patients with periodontal disease or fixed dental work
- Patients in whom intubation is difficult
- If an entire tooth is avulsed, it can be retrieved and saved in moist gauze or normal saline
- With a rapid response from an oral surgeon or dentist, an intact tooth can be re-implanted and saved, usually when performed within 1 hour
- Aspiration is more likely to occur into the right lower lobe
- Because of straighter path and wider bore of right main bronchus
- Aspiration of the tooth may induce serious complications requiring bronchoscopy for removal
- Obstructive pneumonia
- Atelectasis
Other injuries
- Lip injuries
- Lacerations
- Hematomas
- Edema
- Teeth abrasions
- Usually secondary to inattentive laryngoscopy performed by inexperienced practitioners
- Massive tongue swelling (macroglossia) has been reported
- Damage to the uvula (edema and necrosis) usually associated with an endotracheal tube
- Sore throat, odynophagia, painful swallowing have been reported
- Incidence of sore throat after intubation is approximately 40%
- >65% when blood is found on airway instruments
- Trauma to larynx and vocal cords is not uncommon following endotracheal intubation
- In one large study, 6.2% of patients sustained severe lesions to larynx
- Recovery is generally prompt with conservative therapy
- Hoarseness may be present even after a 2-week interval
- Arytenoid dislocation and subluxation have been reported as rare complications

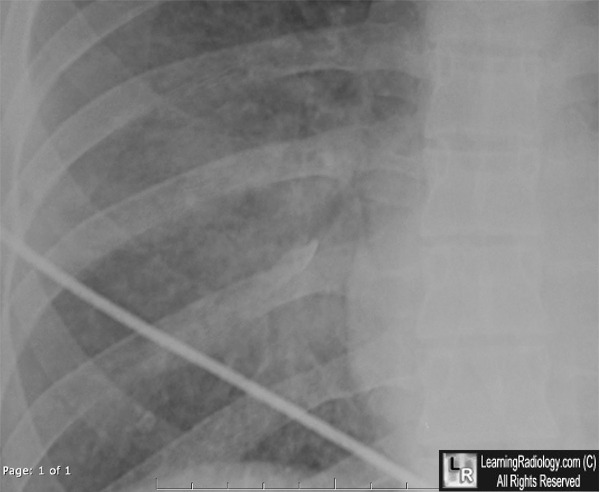
Tooth in Right Lower Lobe Bronchus. Close-up of the right lower lobe on a frontal view of the chest (left) demonstrates a calcified density overlying the right lower lobe (black circle). The patient has pulmonary contusions as a background. An image from an axial CT scan of the chest (right) using "bone "windows clearly shows a tooth in the right lower lobe bronchus (white circle). There is a pulmonary contusion surrounding the tooth. The patient expired from massive head injuries before the tooth could be removed.
For additional information about this disease, click on this icon if seen above.
For this same photo without annotations, click here
|
|
|

{kind=link}