|
|
Free Intraperitoneal Air
Pneumoperitoneum
- Etiology
- Disruption of wall of hollow viscus
- Blunt or penetrating trauma
- Perforating foreign body (eg,
thermometer injury to rectum)
- Iatrogenic perforation
- Laparoscopy / laparotomy (58%)
- Absorbed in 1-24 days depending on
initial amount of air introduced and body habitus (80% in
asthenic, 25% in obese patients)
- Leaking surgical anastomosis
- Endoscopic perforation
- Enema tip injury
- Diagnostic pneumoperitoneum
- Diseases of GI tract
- Perforated gastric / duodenal ulcer
- Perforated appendix
- Ingested foreign-body perforation
- Diverticulitis (ruptured Meckel
diverticulum / sigmoid diverticulum, jejunal
diverticulosis)
- Necrotizing enterocolitis with
perforation
- Inflammatory bowel disease (eg,
toxic megacolon)
- Obstruction* (gas traversing intact
mucosa): neoplasm, imperforate anus, Hirschsprung disease, meconium ileus
- Ruptured pneumatosis cystoides
intestinalis
- Idiopathic gastric perforation =
spontaneous perforation in premature infants (congenital
gastric muscular wall defect)
- Through peritoneal surface
- Transperitoneal manipulation
- Abdominal needle biopsy / catheter
placement
- Mistaken thoracentesis / chest tube
placement
- Endoscopic biopsy
- Extension from chest
- Dissection from pneumomediastinum
(positive pressure breathing, rupture of bulla / bleb, chest
surgery)
- Bronchopleural fistula
- Rupture of urinary bladder
- Penetrating abdominal injury
- Through female genital tract
- Iatrogenic
- Perforation of uterus / vagina
- Culdocentesis
- Rubin test = tubal patency test
- Pelvic examination
- Spontaneous
- Intercourse, orogenital insufflation
- Knee-chest exercise, water skiing,
horseback riding
- Intraperitoneal
- Gas forming peritonitis
- Rupture of abscess
- Air in lesser peritoneal sac gas in
scrotum (through open processus vaginalis)
- Imaging findings
- Large collection of gas
- Abdominal distension, no gastric
air-fluid level
- "Football sign" = large pneumoperitoneum
outlining entire abdominal cavity
- "Double wall sign" = "Rigler sign" = air
on both sides of bowel as intraluminal gas and free air
outside (usually requires >1,000 mL of free intraperitoneal gas + intraperitoneal fluid)
- "Telltale triangle sign" = triangular
air pocket between 3 loops of bowel
- Depiction of diaphragmatic muscle slips
= two or three 6-13 cm long and 8-10 mm wide arcuate
soft-tissue bands directed vertically inferiorly + arching
parallel to diaphragmatic dome superiorly outline of ligaments
of anterior inferior abdominal wall:
- "Inverted V sign" = outline of both
lateral umbilical ligaments (containing inferior epigastric
vessels)
- Outline of medial umbilical ligaments
(obliterated umbilical arteries)
- "Urachus sign" = outline of middle
umbilical ligament
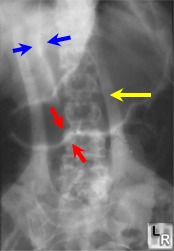
Falciform Ligament Sign. Blue arrows point to falciform
ligament, made visible by a large amount of free air in the peritoneal
cavity.
The red arrows demonstrate both sides of the wall of the stomach (Rigler's
sign), a sign of free air. The yellow arrow points to a skin fold.
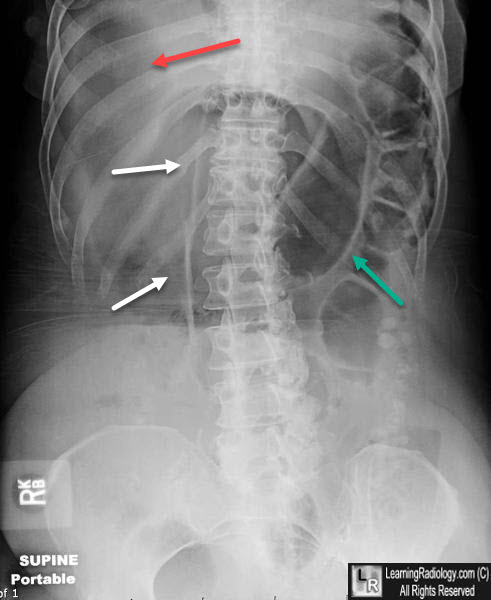
Falciform Ligament Sign (Free Air). White arrows point to falciform
ligament, made visible by a large amount of free air in the peritoneal
cavity.
The green arrow demonstrate both sides of the wall of the bowel wall (Rigler's
sign), a sign of free air. The red arrow points to increased lucency over the liver from a large amount of free air.
- RUQ gas (best place to look for small
collections)
- Single large area of hyperlucency over
the liver
- Oblique linear area of hyperlucency
outlining the posteroinferior margin of liver
- Doge's cap sign = triangular collection
of gas in Morrison pouch (posterior hepatorenal space)
- Outline of falciform ligament = long
vertical line to the right of midline extending from
ligamentum teres notch to umbilicus; most common structure
outlined
- Lligamentum teres notch = inverted V-shaped area of hyperlucency along
undersurface of liver
- Ligamentum teres sign = air outlining
fissure of ligamentum teres hepatis (= posterior free edge of
falciform ligament) seen as vertically oriented sharply
defined slitlike / oval area of
hyperlucency between 10th and 12th rib within 2.5-4.0 cm of
right vertebral border 2-7 mm wide and 6-20 mm long
- "Saddlebag / mustache / cupola sign" =
gas trapped below central tendon of diaphragm
- Parahepatic air = gas bubble lateral to right edge of liver
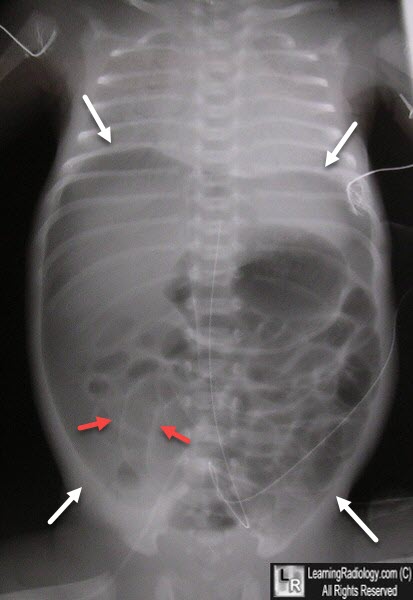
Pneumoperitoneum. There is a very large pneumoperitoneum which renders the entire abdomen more lucent that normal (white arrows). Both sides of the bowel wall are visible (red arrows). The new born also has severe hyaline membrane disease in the chest.
|
|
|
