|
|
Constrictive Pericarditis
- Defined by thickening of pericardium (>4mm) impeding diastolic filling
- Thickened pericardium may calcify (50%)
- Calcified pericardium almost always implies constriction, but not always
- About 50% of calcified pericardiums are visible on conventional radiography
- Calcification of the pericardium is most likely inflammatory in nature
- Can be seen with a variety of infections, trauma, and neoplasms
- Most common causes include
- Viral pericarditis (most common)
- Tuberculous pericarditis
- Uremic pericarditis
- Post-cardiac surgery
- Calcification most commonly occurs along the inferior diaphragmatic surface of the pericardium surrounding the ventricles
- Thin, egg-shell like calcification is more often associated with viral infection or uremia
- Calcification from old TB is often thick, confluent, and irregular in appearance, especially when compared with myocardial calcification
- Calcification is seen in 1/3-1/2 of patients with constrictive pericarditis
- Its presence does not imply constriction
- Must be differentiated from other cardiac calcifications which can usually be done using the locations of these calcifications on multiple views, or the radiographic appearance of the calcium
- Constrictive Pericarditis
- Present when a fibrotic, thickened (>4mm), and adherent pericardium restricts diastolic filling of the heart.
- Usually begins with an initial episode of acute pericarditis
- May not be detected clinically
- This slowly progresses to a chronic stage consisting of fibrous scarring and thickening of the pericardium with obliteration of the pericardial space
- Produces uniform restriction of the filling of all heart chambers
- Reduced cardiac output
- Fatigue
- Hypotension
- Tachycardia
- Elevated systemic venous pressure
- Jugular venous distension
- Hepatomegaly
- Ascites
- Peripheral edema
- Pulmonary venous congestion
- Exertional dyspnea
- Cough
- Orthopnea
- Chest pain typical of angina
- May be due too underperfusion of the coronary arteries, or
- Compression of an epicardial coronary artery by the thickened pericardium.
- Most impressive physical findings are often the insidious development of ascites of hepatomegaly and ascites, such patients are often mistakenly thought to suffer from hepatic cirrhosis or an intra-abdominal tumor
- Calcification of the pericardium is detected in up to 50 % of patients
- This finding is not specific for constrictive pericarditis
- A calcified pericardium is not necessarily a constricted one
- Lateral chest film is useful for its detection in the atrioventricular groove or along the anterior and diaphragmatic surfaces of the right ventricle.
- Pleural effusions are present in about 60 % of patients
- Persistent unexplained pleural effusions can be the presenting manifestation
- CT or MRI are superior in the assessment of pericardial anatomy and thickness
- If the pericardium is calcified, then it is not restrictive cardiomyopathy
- If the pericardium is normal, the it is not constrictive pericarditis
- Differentiating constrictive pericarditis from restrictive cardiomyopathy
- Clinically may resemble each other
|
Constrictive
Pericarditis |
Restrictive Cardiomyopathy |
Heart size |
Normal |
Normal |
Pericardial Thickening |
Required |
Excludes |
Pericardial Calcification |
About 50% of time |
Absent |
- Treatment for constrictive pericarditis can include complete resection of the pericardium

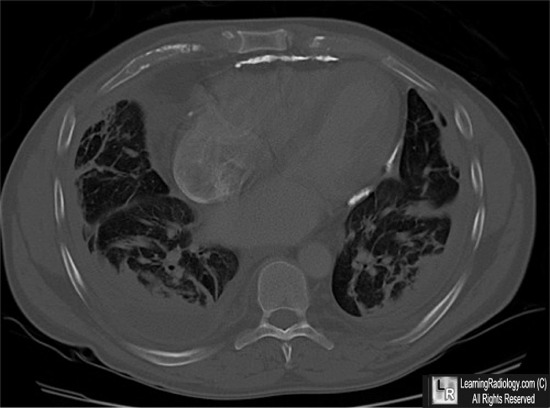
Constrictive Pericarditis. This axial CT image of the chest is displayed using bone windows to show the calcifications of the pericardium (red arrows).
There are bilateral pleural effusions present (white arrows), a common finding in constrictive pericarditis.
For this same photo, click here
For more information, click on the link if you see this icon 
|
|
|

{kind=link}