|
Substernal Thyroid Goiter
• Extension of a thyroid goiter arising in the neck inferiorly into the thorax is relatively uncommon
• Most (75-80%) arise from lower pole or isthmus of the thyroid and extend into anterior mediastinum
• Some arise from posterior aspect of the thyroid and extend into posterior mediastinum, almost always on the right
• Usually nodular, colloid goiters
•Thyrotoxicosis and carcinoma are rare
• Thyroid mass is typically well-encapsulated and may show degeneration (calcification)
• Most patients are asymptomatic
Imaging
• Sharply defined, smooth or lobulated soft tissue mass which characteristically displaces the trachea
• They do not usually project below the arch of the aorta differentiating them from thymomas and teratomas
• Those in the posterior mediastinum characteristically interpose between the trachea in front and the esophagus in back
• On CT, they usually contrast enhance and many times are found to contain calcification.
• Curvilinear calcifications are highly suggestive of a degenerated thyroid adenoma
• Radioisotope scan is diagnostic
Substernal Thyroid Goiter. Contrast-enhanced CT of the chest shows a large, contrast-enhancing
mass in the anterior mediastinum containing calcifications and areas of necrosis.
For the same photo, click here
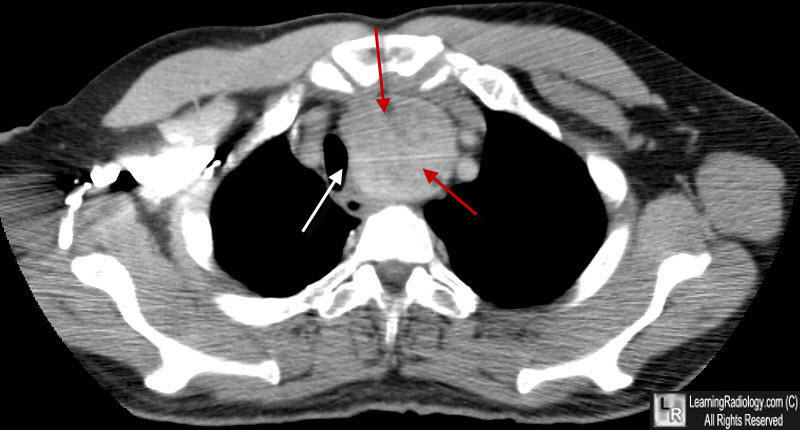
Substernal Thyroid Goiter. Contrast-enhanced CT of the chest shows a large, contrast-enhancing
mass in the anterior mediastinum (red arrows) displacing the trachea (White arrow) to the right.
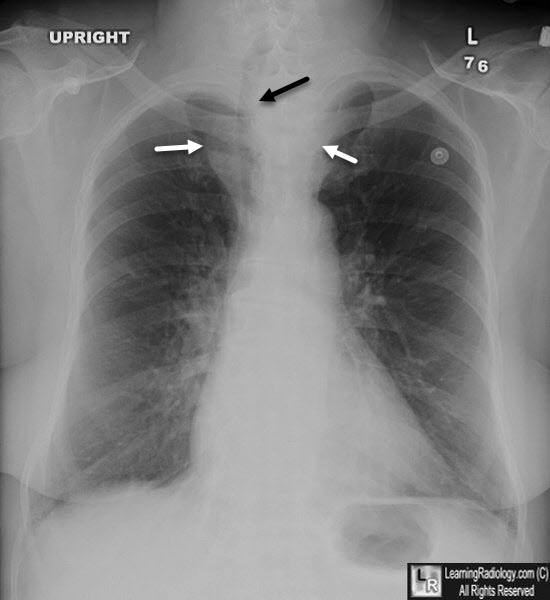
Substernal Thyroid Goiter. Frontal chest radiograph shows a large superior/anterior mediastinal mass (white arrows) displacing the trachea (black arrow) to the right of midline.
|

