|
Fractures of the Proximal Femur
Femoral Neck Fractures
· Hip fractures are associated with a substantial mortality, as many as 15-20% dying within one year of the fracture
· Conditions that predispose to hip fractures include aging, osteoporosis and osteomalacia
o Most hip fractures in the elderly (90%) occur as a result of a fall, frequently a minor fall such as from the standing position
· In younger individuals, hip fractures are often the result of high velocity, high impact trauma
· Most hip fractures occur in Caucasian women
· Imaging
o Conventional radiography is the study of first choice
o When further imaging is required, MRI or nuclear medicine scans are used most often utilized
o The femoral neck will be seen in profile when the leg is held in internal rotation
· Hip fractures can be classified as to their geographic position as: subcapital, transcervical, basicervical, intertrochanteric and subtrochanteric
o Subcapital, transcervical and basicervical are intracapsular
o Intertrochanteric and subtrochanteric are extracapsular
· Intracapsular fractures have a higher incidence of nonunion and avascular necrosis of the femoral head (up to 35%) than extracapsular fractures
o The more displaced the fragments are, the higher the rate of complications
· Subcapital fractures
o Most common intracapsular fracture of the hip
o Subtle, frequently impacted
o White line of increased density of impacted bone may be seen at base of femoral head
o There may be a discontinuity in the normal smooth curve of the superior aspect of the femoral neck as it joins the head
o Pitfall: a rim of osteophytes may form around the femoral head and project over the neck mimicking the sclerotic line of a subcapital fracture
§ Look for cortical discontinuity
§ May require additional imaging such as MRI for confirmation of fracture
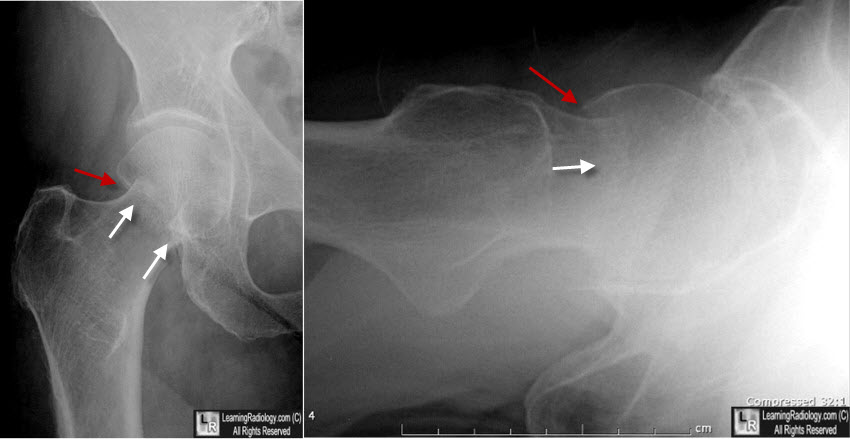
Sub-capital hip fracture. On the frontal view, there is a step-off in the cortex superiorly (red arrow) while there is abnormal overlapping of the femoral head and neck (white arrows) due to impaction. On the lateral view, the same step-off can be seen (red arrow) as well as the impaction (white arrow).
· Transcervical fractures
o Occur across the neck of the femur
o Usually easy to see on views of the hip obtained in internal rotation
o Frequently associated with varus deformity
· Basicervical fractures
o Base of the femoral neck
o May be difficult to differentiate a basicervical fracture from a non-displaced and non-comminuted intertrochanteric fracture
· Intertrochanteric fractures
o Most common of the extracapsular hip fractures
o Comminuted fractures may also manifest separate fragments of either or both of the lesser and greater trochanters
o Intertrochanteric fractures associated with a separate fragment of lesser trochanter may also include a portion of the posterior cortex of femoral neck and are considered unstable
o Many intertrochanteric fracture are associated with a varus deformity
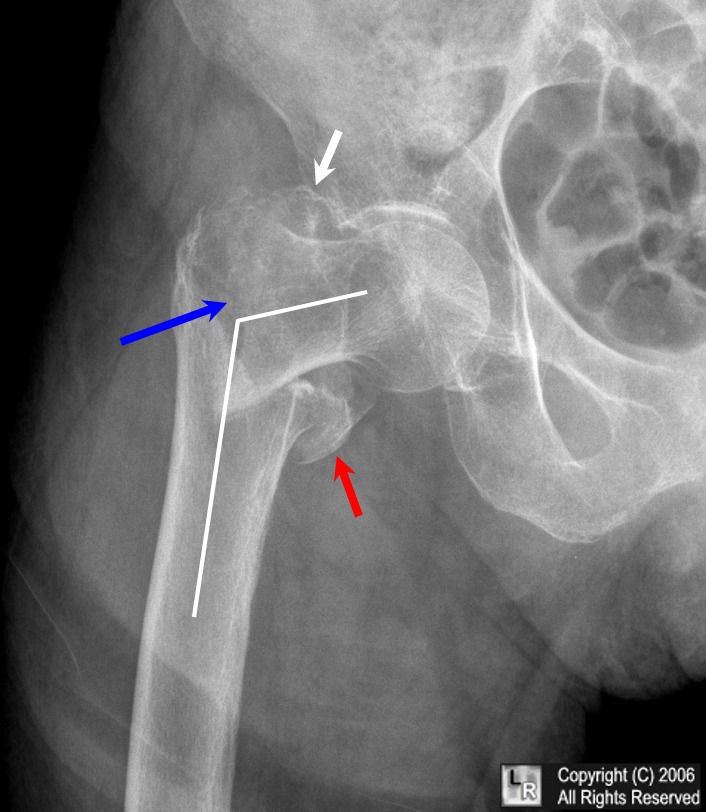
Comminuted intertrochanteric fracture. There is a fracture from the
greater to the
lesser trochanter (blue arrow). There are separate fragments of the greater trochanter
(white arrow) and lesser trochanter (red arrow). There is varus deformity
(white line) of the femoral shaft.
For a larger photo of the same image without arrows, click on this link
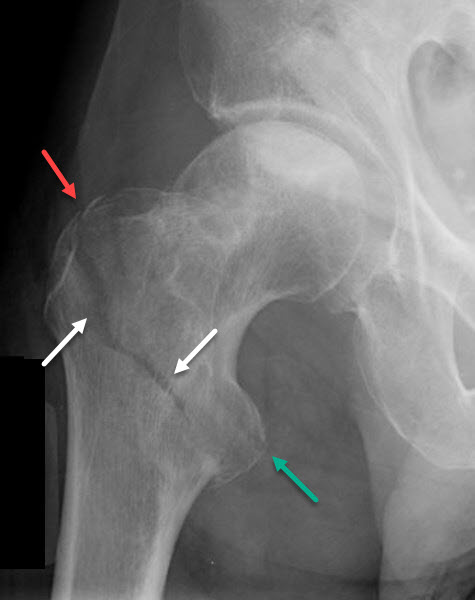
Intertrochanteric fracture. There is a fracture from the
greater (red arrow) to the
lesser (green arrow) trochanter. A lucency, representing the fracture, runs between the two trochanters (white arrows).
· Isolated fractures of the greater trochanter
o Occur in osteoporotic females and are the result of a fall on the greater trochanter or may occur as an avulsion-type fracture from pull of the gluteus medius insertion
o These fractures may be difficult to see as the greater trochanter may be overexposed on routine views of the hip
o Important to exclude an intertrochanteric fracture which requires operative reduction and internal fixation, while the isolated fracture of the greater trochanter does not
o MRI may be needed to exclude intertrochanteric extension
· Classification - Garden Classification
o The most commonly used classification system for femoral neck fractures is some variation of the Garden classification
o As its basis, the classification separates non-displaced fractures from displaced fractures because of the better healing rate of the former
Stage |
Description |
Remarks |
Stage I |
Incomplete fracture of the neck |
May be impacted and in valgus |
Stage II |
Complete without displacement |
|
Stage III |
Complete with partial displacement |
Fragments are still connected by posterior retinacular attachment |
Stage IV |
Complete femoral neck fracture with full displacement |
Allows the femoral head to rotate back into anatomical position |
· Treatment
o Intracapsular fractures of the femoral neck are most often treated with a prosthetic or replacement device for the femoral head and/or neck
o Intertrochanteric fractures are frequently treated using a compression-type screw, pin or nail and laterally-placed side-plate
§ Intramedullary nails are also used for fixation
|

{kind=link}