|
Bullous Disease of the Lungs
· Definition
o Thin-walled–less than 1 mm
o Air-filled space
o Contained within the lung
o 1 cm in size when distended
o Walls may be formed by pleura, septa, or compressed lung tissue
· What a bulla isn’t: other air-containing structures
o Pneumatocoele
§ Thin-walled (< 1mm), gas-filled space in the lung developing in association with acute pneumonia, such as staph, and frequently transient
o Cavity
§ Gas-containing space in the lung having a wall > 1 mm thick
o Cyst
§ Thin-walled, air- or fluid-filled, with a wall that contains respiratory epithelium, cartilage, smooth muscle and glands
o Bleb
§ Intrapleural cystic space
· Bulla terminology
o One of them is a bulla
o Two or more of them are bullae (pronounced bully)
o Diseases which contain bullae are bullous diseases
· General considerations
o Enlarge progressively over a period of months to years
o Most are associated with emphysema
o May become infected or lead to pneumothorax
· Primary Bullous Disease
o Familial occurrence
o Increased incidence in Marfan's and Ehlers-Danlos
o Unlike the bullae associated with emphysema, there is usually no airway obstruction and there is normal parenchyma between bullae
· Types of Bullae
o Type 1
§ Originate in a subpleural location usually in upper part of lung
§ Narrow neck
§ Produce passive atelectasis of adjacent lung tissue
§ Paraseptal emphysema
o Type 2
§ Superficial in location
§ Very broad neck
§ Anterior edge of upper and middle lobes and along diaphragm
§ Contain blood vessels and strands of partially destroyed lung
§ Spontaneous pneumothorax
o Type 3
§ Lie deep within lung substance
§ Like type 2, contain residual strands of lung tissue
§ Affect upper and lower lobes with same frequency
· Imaging findings
o Seen more in upper lobes
o Thin-walled, sharply demarcated areas containing no visible blood vessels on conventional radiography
o Only portion of wall is usually seen on conventional radiography
o They tend to trap air
§ May become larger on expiration
o Bullae may become so large as to render the remaining normal lung almost invisible, pancaked atop the hemidiaphragm = vanishing lung syndrome
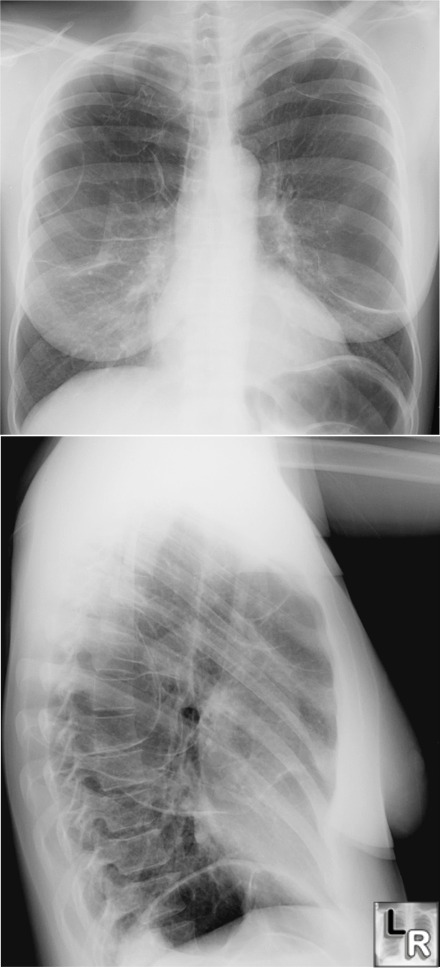

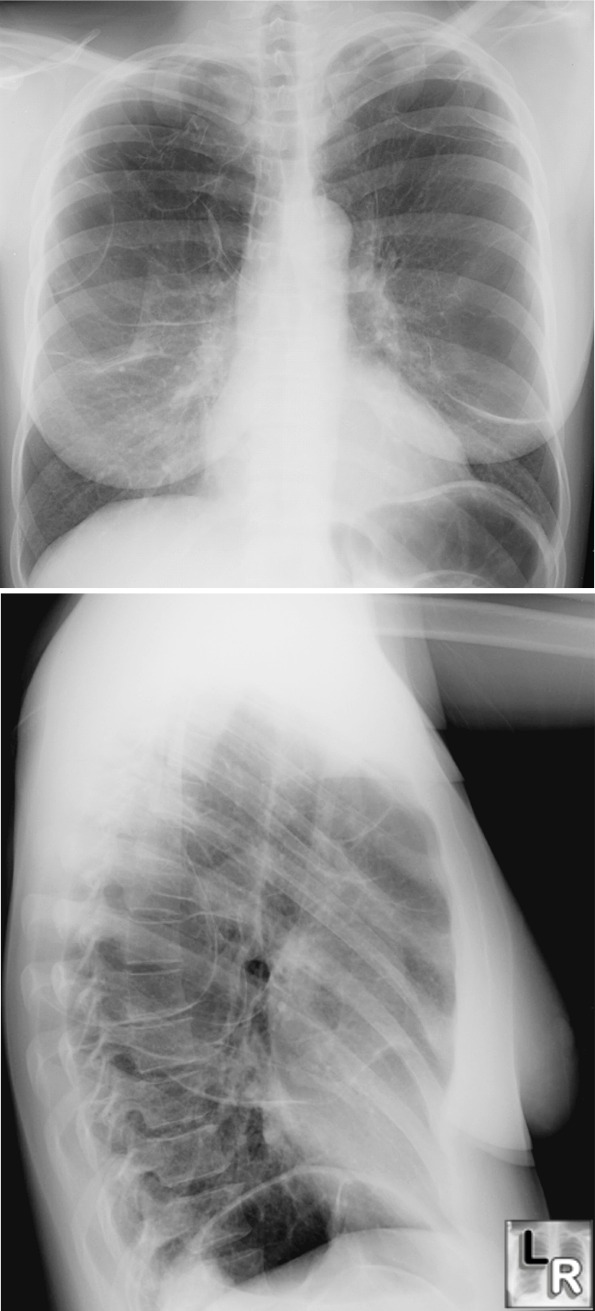
Bullous disease of the lungs-conventional radiograph and CT. Frontal
and lateral views of the chest
demonstrate
numerous thin-walled,
air-containing structures that represent the walls of numerous bullae.
These lineal densities
are characteristic for bullae on conventional
radiography. The CT scan on the same patient (below) shows the
same thin-walled bullae.
For larger photos of the same images, click on the photos above
· Signs of an infected bulla
o Air-fluid level
o Differentiation from lung abscess
§ Bulla contains less fluid
§ Much thinner wall
§ No surrounding pneumonitis
§ Patients less sick with infected bulla
o Clearing may take weeks to months
· Bullous disease and spontaneous pneumothorax
o Commonly occurs with small bulla affecting lung apices
o May be difficult to differentiate large bulla from pneumothorax
o Edge of a pneumothorax will usually parallel the chest wall curvature whereas edge of a bulla frequently curves inwards away from the chest wall
o CT may help
· Clinical findings
o 1° bullous disease usually has no symptoms
o When large, surgical removal may be performed
o Patients with chronic obstructive pulmonary disease tend to show little difference clinically or functionally with or without bullae
|