|
|
Bezoar
General Considerations
- Collections of indigestible material found in the gastrointestinal tract, usually the stomach
- From the Persian word “padzahr” which means antidote since they were once used for this purpose
- Incidence is very low
- Risk of trichobezoar (eating of hair) is greater among mentally challenged or emotionally disturbed children
- Also occurs as an occupational disease in brushmakers, blanket weavers and wool workers
- Much more common in females (90%) aged 10 to 19
Etiology
- Chewing on or eating hair or fuzzy materials or indigestible vegetable fiber
- Material unable to exit stomach because of large size
- Gastric outlet obstruction may play a roll
- Poor gastric motility such as might occur in diabetics also may contribute
Predisposition
- Previous gastric surgery such as vagotomy, pyloroplasty, antrectomy or partial gastrectomy
- Inadequate chewing of food
- Massive overindulgence of food with high fiber contents such as dates or persimmons
Clinical symptoms
- Anorexia
- Bloating
- Early satiety
- History of trichophagy – eating hair
- Trichoptysis – hair may be coughed up
- May be asymptomatic
Phytobezoar (55% of all bezoars):
- Poorly digested vegetable fibers such as
- Skin and seeds of fruits and vegetables
- Oranges
- Persimmons
- Most common
- Unripe persimmons contain a chemical “shibuol” that forms a gluelike coagulum after contact with dilute acid in the stomach
- May become impacted in small bowel after forming in stomach
Trichobezoar (hair)
- 80% are < age 30, almost exclusively in females
- Associated with gastric ulcer in 24-70%
Imaging findings
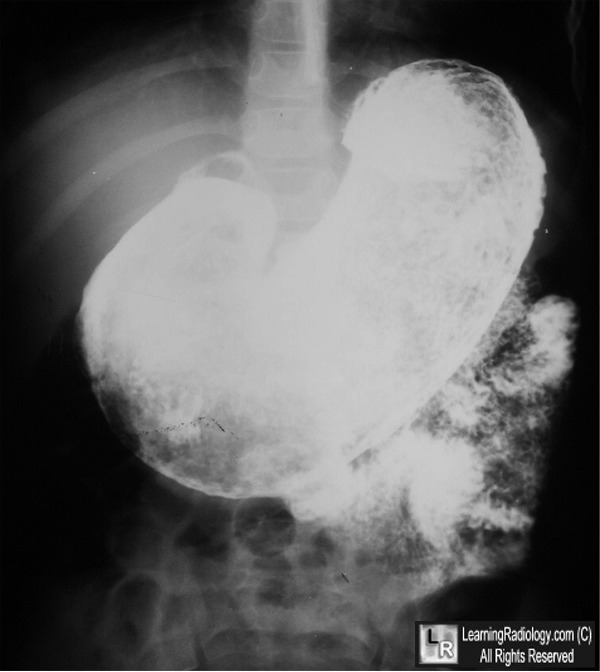
- Upper part of a large bezoar may be visible as a mass with a convex upper border projecting into the gastric air bubble
- An erect abdominal radiograph and a supine radiograph may show a prominent gastric outline with an intragastric mottled mass, outlined by gas in the distended stomach, mimicking a food-filled stomach
- On barium studies, they produce an intraluminal filling defect without attachment to bowel wall
- Interstices of bezoar are filled with barium
- Barium remains in bezoar for hours after exiting remainder of bowel
- Get delayed film if bezoar is suspected
- Partial or complete bowel obstruction
- CT
- Mobile intragastric mass consisting of "compressed concentric rings"
- A mixed density pattern due to the presence of entrapped air and food debris
Complications
- Pressure necrosis of bowel wall may lead to perforation, peritonitis
- Distal extension of the bezoar can lead to
- Obstructive jaundice
- Acute pancreatitis
- Protein-losing enteropathy
- Steatorrhea
- Mechanical small bowel obstruction alone or with perforation
DDx
- Lobulated, villous adenoma
- Leiomyosarcoma

Bezoar. A huge filling defect with barium intermixed in its
interstices is seen in the dilated stomach of this patient with a bezoar (blue arrow).
The image is from an upper gastrointestinal series.
For these same photos without the arrows, click here
For more information, click on the link if you see this icon 
Gastric Trichobezoar - Narinder K Kaushik, Yash P Sharma, Asha Negi, Amal Jaswal: Ind J Radiol Imag 1999; 9 : 3 : 137-139
|
|
|

{kind=link}