|
|
Emphysematous Cholecystitis
- General considerations
- Acute infection of gallbladder caused by gas-forming organism
- In about 1/3 = clostridium perfringens
- Also E. Coli and Klebsiella
- Rare – only 1% of all cases of acute cholecystitis
- Occurs more often in men
- As opposed to gallbladder disease in general which occurs more often in women
- Mostly are elderly patients (>60) with diabetes
- Vascular compromise of the cystic artery may play a role in the etiology
- Gallstones may be associated with the disease but are not thought to cause it
- Gas may occur in the wall and/or the lumen
- May spread to pericholecystic tissue
- Rarely, gas may escape into the bile ducts
- This is rare since cystic duct is usually occluded in cholecystitis
- Clinical findings
- As with cholecystitis, right upper quadrant (RUQ) pain and tenderness
- Leukocytosis
- Jaundice is rare
- Imaging findings
- Conventional radiography
- May show air in the wall or lumen of the gallbladder
- Air-fluid levels in the gallbladder will only be seen with images obtained with a horizontal beam, not on supine radiographs
- Gas may spread to the pericholecystic tissues
- These findings, if present on the conventional radiograph, usually herald a poor outcome from late-stage disease
- US findings
- Indistinct shadowing emanating from wall or lumen of gallbladder
- “Ring-down effect” or “comet tail” from shadowing from air in gallbladder lumen
- CT findings of cholecystitis
- Air in gallbladder wall is diagnostic of this disease
- Most common signs of non-emphysematous cholecystitis are gallbladder wall thickening >3mm, and
- Cholelithiasis
- Increased density of bile (>20 H)
- Loss of clear definition of gallbladder wall
- Pericholecystic fluid such as a halo of edema
- Treatment
- Definitive care involves surgical intervention
- Preoperative percutaneous drainage may improve survival
- Emergency cholecystectomy
- Complications
- Fivefold increase in perforation over uncomplicated acute cholecystitis
- Perforation of the gallbladder
- Frequency is declining because of earlier diagnosis of acute cholecystitis
- Diagnosis
- Pre-perforation conventional radiograph showing stones clustered in gallbladder may subsequently show stones scattered in RUQ after perforation
- Pericholecystic fluid collection on CT or US (not-specific)
- Scintography may show radiotracer outside of gallbladder in Morrison’s pouch or flank
- Treatment
- Preoperative percutaneous drainage of gallbladder and biloma
- Emergency surgery

Emphysematous Cholecystitis. Supine view of the abdomen shows air in the wall (blue arrows) of the gallbladder (GB). There is also a lucency within the lumen of the gallbladder (GB) suggesting air inside the lumen. There is no air-fluid level visible because this radiograph is obtained supine with a vertical x-ray beam. Just superior to the gallbladder is another collection of air (red arrow) that represents a pericholecystic abscess. The yellow arrow points to the end of a PEG tube in the stomach.
For this same photo without the arrows, click here
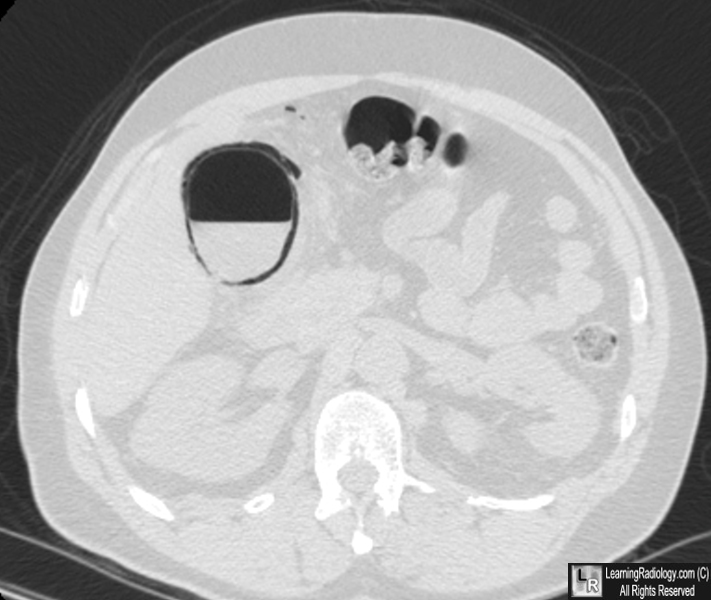
Air is contained both within the gallbladder lumen (see air-fluid level) and the wall of the gallbladder (curvilinear lucency surrounding gallbladder).
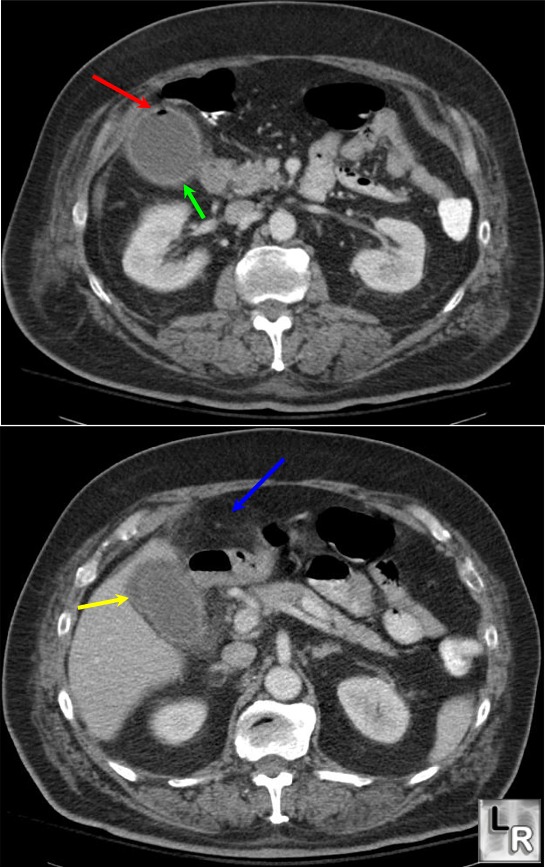
Emphysematous cholecystitis-red arrow points
to air in lumen of gallbladder; green arrow
points to thickened gallbladder wall; blue arrow points to
pericholecystic stranding;
yellow arrow points to pericholecystic fluid
Gore, R. and Levine, M: textbook of Gastrointestinal; Radiology, W.B. Saunders, 2000.
Moss, A., Gamsu, G. and Genant, H.: Computed Tomography of the Body. W.B. Saunders,1992.
|
|
|

{kind=link}
{kind=link}