|
|
Coarctation of the Aorta
General
o 2X more common in males
Common classification
o Infantile or preductal form
o Adult or juxtaductal form
Adult Form
o Adult or juxtaductal (postductal) form is more common
o Usually localized
o Area of coarctation is just beyond the origin of LSCA at level of
ductus
Infantile Form
o Infantile, preductal form = diffuse type
o Long, tubular segment of narrowed aorta
§ From just distal to innominate to level of ductus
o Intracardiac defects (VSD,ASD, deformed
mitral valve) present in 50% of diffuse type
§ Also patent ductus arteriosis
Other Classifications
o More complicated classifications take following into account:
§ Location and length of coarct
§ Patency of ductus arteriosis
§ Relationship of coarct to ductus
Associated Defects
o Bicuspid aortic valve (most common associated defect seen in 75-80%)
o VSD
o ASD
o Transposition
o Found in 25% of patients with Turner’s Syndrome
Shone Syndrome
o Coarctation
o Aortic stenosis
o Parachute mitral valve
o Supravalvular mitral ring
Imaging findings
o Rib Notching
§ Single best sign
§ Older the person, more likely to have rib notching
§ Majority have it over 20 years of age
§ Rib notching occurs in the high pressure circuit
§ Most often involves 4th-8th rib
· Sometimes may involve 3rd and 9th
· Does not involve 1st and 2nd ribs
· Intercostals come off costocervical trunk and do not supply
collateral flow to descending aorta
§ 4th-8th do anastomose with internal mammary to form collaterals for
descending aorta
§ Rib Notching–Unilateral
· Isolated Right sided notching occurs when LSCA is involved in actual
coarctation
· Isolated Left sided notching can occur if there is an aberrant RSCA
which arises from below coarct
o Figure 3 Sign
§ Caused by (in order) either a dilated LSCA or aortic knob,
“tuck” of coarct itself, and poststenotic dilatation
§ Occurs in 1/3–1/2 of patients with coarct
§ Matched by “reverse 3” or “E” on barium-filled esophagus
o Convexity of left side of mediastinum just above aortic knob 2° to
dilated LSCA
o Convexity of ascending aorta in 1/3
Clinical Findings–Infancy
o Severe CHF most common from 2nd to
6th week of life
o Weak or absent leg pulses
o Lower BP in the legs than in the arms
o EKG
§ RV hypertrophy because RV assumes most of the cardiac output during
fetal life in these patients
Clinical Findings-Children and Adults
o Differential pulses in arms (bounding) and legs (weak)
o EKG
§ LVH
Echocardiographic Findings
o 2D echo can demonstrate coarcts from suprasternal notch
o Echo is most helpful in excluding associated hypoplastic left heart
syndrome
Complications
o Heart failure in neonate
o Subarachnoid bleeds from ruptured Berry aneurysms
o Dissection of aorta
o Infective endocarditis
o Mycotic aneurysm
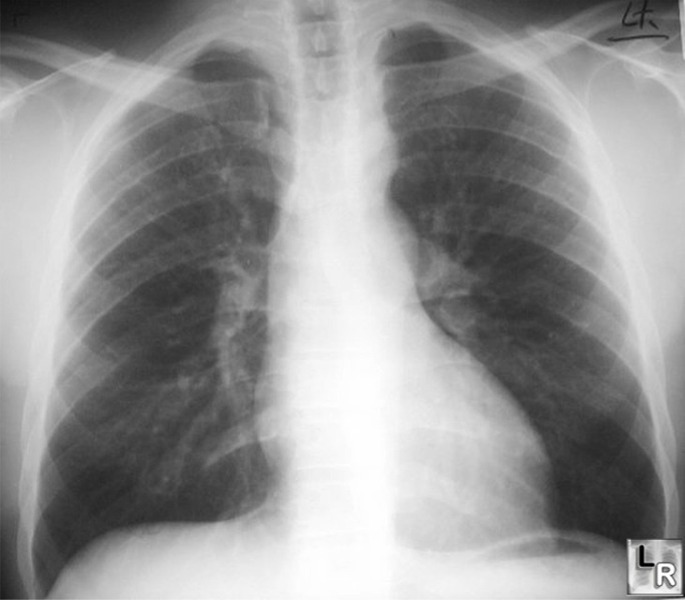
Coarctation of the Aorta. See close-up image below.
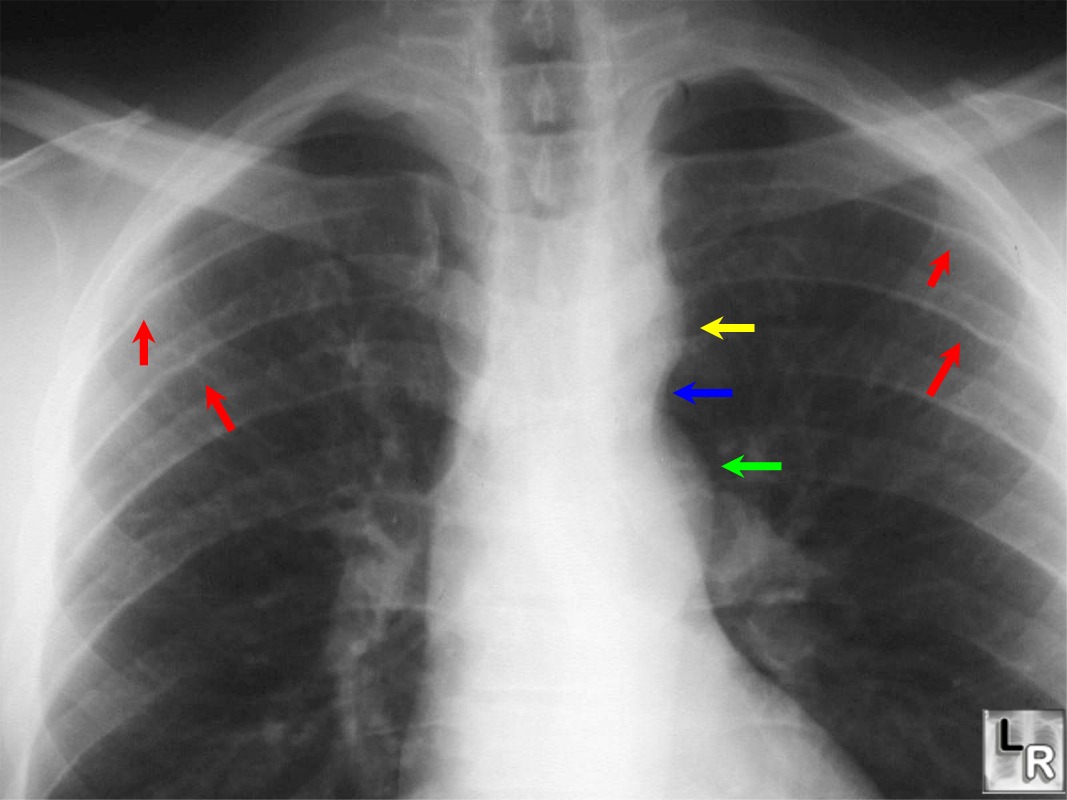
Coarctation of the Aorta. Close up of upper
thorax in a patient with Coarctation of the Aorta.
The red arrows point to rib notching caused by the dilated intercostal
arteries.
The yellow arrow points to the aortic knob, the blue arrow to the
actual coarctation
and the green arrow to the post-stenotic dilation of the descending
aorta.
|
|
|
