|
|
Sigmoid Volvulus
General Considerations
- Twisting of loop of intestine around its mesenteric attachment site may occur at various sites in the GI tract
- Most commonly: sigmoid & cecum
- Rarely: stomach, small intestine, transverse colon
- Results in partial or complete obstruction
- May also compromise bowel circulation resulting in ischemia
- Sigmoid volvulus most common form of GI tract volvulus
- Accounts for up to 8% of all intestinal obstructions
- Most common in elderly persons (often neurologically impaired)
- Patients almost always have a history of chronic constipation
Pathophysiology
- Redundant sigmoid colon that has a narrow mesenteric attachment to posterior abdominal wall allows close approximation of 2 limbs of sigmoid colon à twisting of sigmoid colon around mesenteric axis
- Other predisposing factors
- Chronic constipation
- High-roughage diet (may cause a long, redundant sigmoid colon)
- Roundworm infestation
- Megacolon (often due to Chagas dz)
- 20-25% mortality rate
- Peak age > 50 yrs.
- Second largest group à children
- Torsion usually counterclockwise ranging from 180 – 540 degrees
- Luminal obstruction generally @ 180 degrees
- Venous occlusion generally @ 360 degrees à gangrene & perforation
- Signs and symptoms
- May present as abdominal emergency
- Acute distension
- Colicky pain (often LLQ)
- Failure to pass flatus or stool (constipation is prevailing feature)
- Vomiting is late sign
- Distention may compromise respiratory & cardiac function
- May also present with surprisingly few signs and symptoms in bedridden and debilitated
- Physical examination
- Tympanitic abdomen
- Abdominal distention
- +/- palpable mass
Diagnosis
- Abdominal plain films usually diagnostic
- Inverted U-shaped appearance of distended sigmoid loop
- Largest and most dilated loops of bowel are seen with volvulus
- Loss of haustra
- Coffee-bean sign à midline crease corresponding to mesenteric root in a greatly distended sigmoid
- Sigmoid volvulus – bowel loop points to RUQ
- Cecal volvulus – bowel loop points to LUQ

- Bird’s-beak or bird-of-prey sign à seen on barium enema as it encounters the volvulated loop
- CT scan useful in assessing mural wall ischemia
Differential Diagnosis
Treatment
- Laparoscopic de-rotation or laparotomy +/- bowel resection
- De-rotation & decompression by barium enema or with rectal tube, colonoscope, or sigmoidoscope if no signs of bowel ischemia or perforation
- Cecopexy à suture fixation of bowel to parietal peritoneum may prevent recurrence
- Recurrence rate after decompression alone à 50%

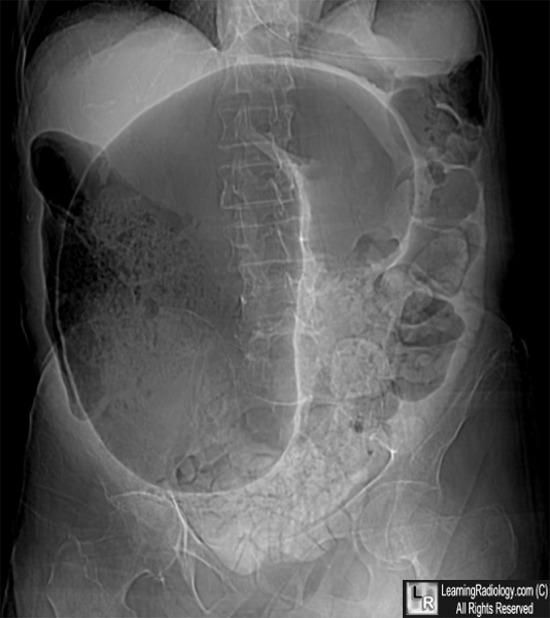
Sigmoid Volvulus. Dilated loop of sigmoid colon has a "coffee-bean" shape and
the wall between the two volvulated loops of sigmoid (black arrow) "points" towards the right upper quadrant.
There is a considerable amount of stool in the colon from chronic constipation.
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here
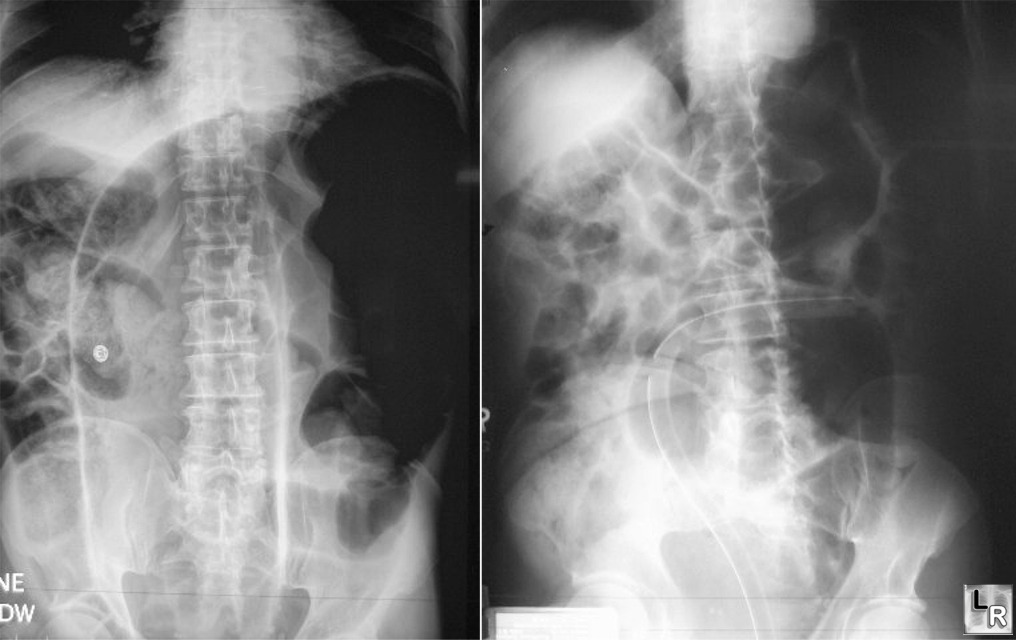
Sigmoid Volvulus. Photo on left shows large, dilated loop of large
bowel with an inverted U-shape
with walls between two volvulated loops pointing from LLQ toward RUQ;
Photo on right shows same patient with decompressed sigmoid volvulus
following insertion of rectal tube
|
|
|

){kind=link}
){kind=link}
{kind=link}