|
|
Adrenal Adenoma
Submitted by Shuchi Rodgers, MD
- Incidence in the
population is 2-8%
- Diagnosis is
often made as an incidental finding on CT examination.
- In patient with
no known primary, an adrenal mass is almost always a benign adenoma
- In a patient
with a known neoplasm, especially lung cancer, an adrenal mass is
problematic and diagnosing a metastasis versus an adenoma is critical
for prognosis
Imaging
findings
- CT
- Size greater
than 4 cm tend to be metastases or adrenal carcinoma
- Heterogeneous appearance and irregular shape are malignant
characteristics
- Homogeneous
and smooth are benign characteristics.
- Intracellular lipid in adenoma results in low attenuation on CT
- Little intracytoplasmic fat in metastases
results in high attenuation on non-enhanced CT
- Non-enhanced
CT (NECT)
- Threshold 10
HU
- Sensitivity
79%, specificity 96%
- Contrast-enhanced CT (CECT)
- Because
majority of CT examinations in oncology use IV contrast, the %
washout is useful after 10 minutes.
- Adenomas
have greater than 50% washout after 10 minutes
- Washout can
also be used on adrenal masses that measure > 10 HU on NECT
- Alternative
is to do MR or PET
- MR
- Chemical Shift
- Most
sensitive method for differentiating adenomas from metastases
- Sensitivity
81-100%. Specificity 94-100%.
- The
difference in resonance rate of protons in fat and water is
exploited in chemical shift.
- Intracellular lipid and water in same voxel result in summation
of signal on "in-phase" and canceling out of signal on "out of
phase"
- Spleen or
muscle is used as an internal standard to visually quantify signal
drop-off
- Liver is not
a reliable standard because of steatosis
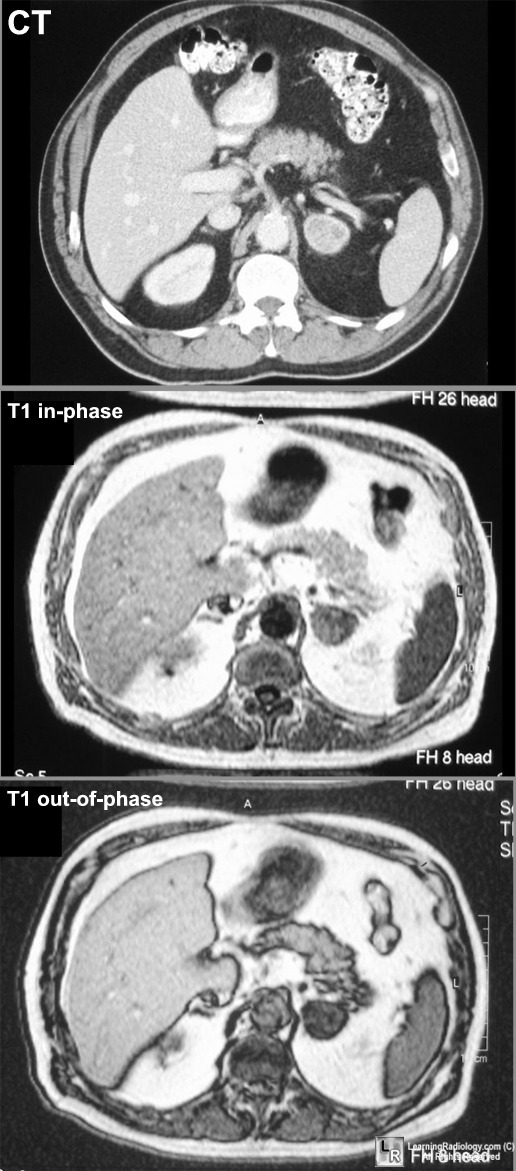
CT shows left adrenal mass.
In-phase T1 shows adrenal mass is hyperintense relative to the spleen.
T1 out-of-phase shows adrenal mass is hypointense to the spleen and
compared to the
in-phase, there is a drop in signal intensity
|
|
|
