|
|
Persistent Left Superior Vena Cava
- Incidence-uncommon
- 0.3% of general population;
- 4.3-11% of patients with CHD
- Two types
- Persistent left SVC connecting to right atrium
via coronary sinus is only common anomaly of SVC (90% of this
anomaly)
- In other 10%, persistent SVC connects to left
atrium
- Most with connection to left atrium have
associated ASD or heterotaxy syndromes
- This produces a right-to-left shunt of a
rather small magnitude
- Etiology
- Failure of regression of left anterior and
common cardinal veins and left sinus horn
- Course of persistent left SVC
- Draining into right atrium
- Starts at junction of left subclavian vein
and left internal jugular
- Passes lateral to aortic arch
- Receives left superior intercostal vein
- Anterior to left hilum
- Joined by hemiazygos system
- Crosses posterior wall of left atrium
- Receives great cardiac vein to become
coronary sinus (common)
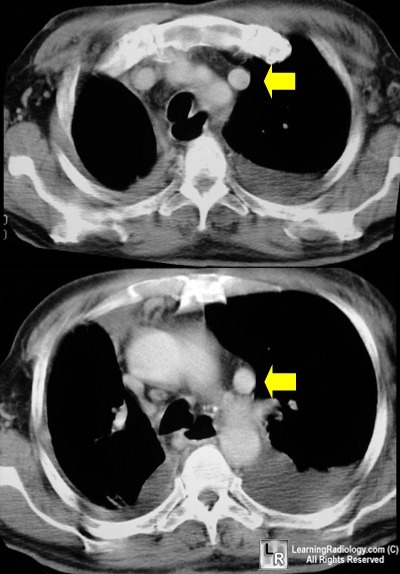
Yellow arrows point to left-sided persistent SVC
passing lateral to aortic arch and anterior to left hilum
- Draining into left atrium
- Starts at junction of left subclavian vein and
left internal jugular
- Passes lateral to aortic arch
- Receives left superior intercostal vein
- Anterior to left hilum
- Joined by hemiazygos system
- Passes between the left atrial appendage
(anteriorly) and the left superior pulmonary vein posteriorly
- Absent / small left brachiocephalic vein (65%)
- Really this abnormality produces bilateral SVCs
- In small percentage, right SVC is absent
(10-18%)
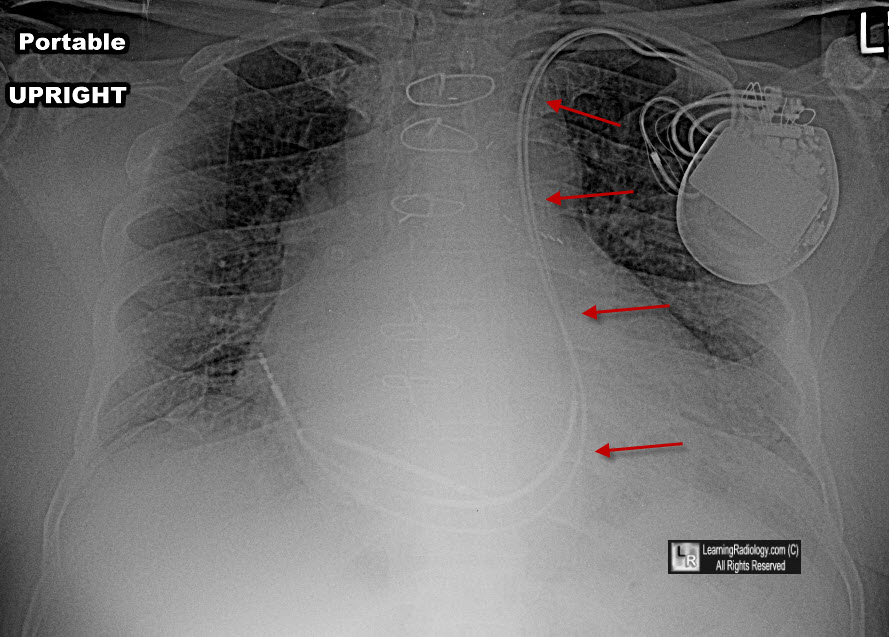
The leads of the AICD enter the left subclavian vein and subsequently drain into a persistent left superior vena cava (red arrows) and from there into right atrium and right ventricle.
Freedom, Culham and Moes, Angiography
of Congenital Heart Disease, 1984
|
|
|
