|
Boerhaave Syndrome
General Considerations
•
Nearly all esophageal perforations are caused by trauma
• Causes include:
> Iatrogenic–endoscopy (about 75% of the perforations in adults), dilatation
procedures
> Stab wounds
> Occasionally, blunt compression of the chest
> Severe vomiting or straining
•
Non-traumatic causes include neoplasm or caustic ingestion
•
In infants, the most frequent site of rupture is the cervical esophagus 2°
passage of tubes
Boerhaave's
Syndrome
• Usually in men, although neonatal esophageal rupture occurs primarily in
girls
• Associated with the clinical triad of vomiting, chest pain and
subcutaneous/mediastinal emphysema
• In neonates, there is cyanosis and dyspnea associated with a right tension
pneumothorax immediately after birth
• In Boerhaave’s, the inciting cause may be vomiting, straining, childbirth
or a blunt blow to the abdomen or thorax
• Tears are vertically oriented, 1-4 cm in length
• Almost all (90%) occur along the left posterolateral wall of the distal
esophagus
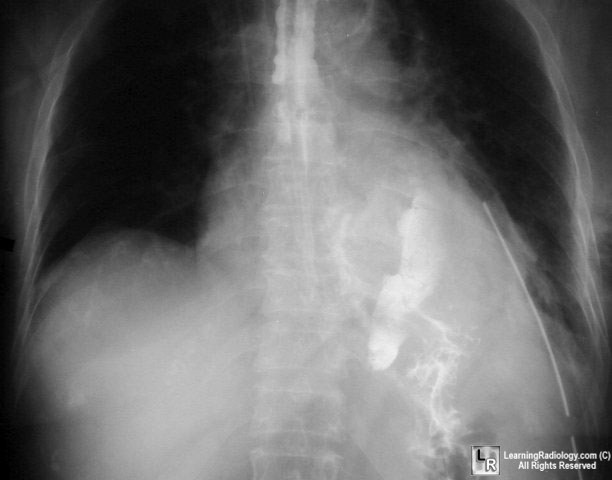
Photo shows extraluminal contrast
arising from left, posterolateral tear of esophagus
Imaging
• Mediastinal emphysema
• Left pleural effusion
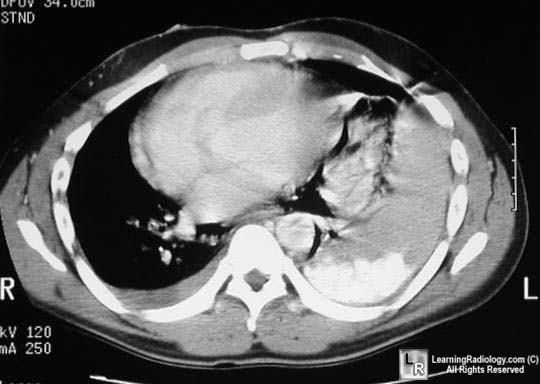
Photo shows mediastinal emphysema and
extraluminal contrast in pleural space on left
• Mediastinal widening
• Subcutaneous emphysema
• Nacleiro sign-a V-shaped radiolucency seen through the heart
representing air in the left lower mediastinum that dissects under the left
diaphragmatic pleura
• In neonatal rupture, pneumomediastinum is uncommon
• Method of study:
• First use a water-soluble contrast agent (Gastrografin, oral Hypaque)
• If no perforation is found, then barium may be used
|
