|
|
Dermoid Cyst of the Ovary
Teratoma
General Considerations
- Dermoids, a term now used almost always interchangeably with teratomas, are tumors
derived from more than one germ layer, frequently all three
- As such, they can include hair, teeth, fat, skin, muscle, endocrine tissue
- Ectodermal tissue predominates
- Mature cystic teratomas are commonly referred to as dermoid cysts
- They are the most common ovarian neoplasm
- Mature cystic teratoma of the ovary is invariably benign
- In rare cases (1-3%), they may undergo malignant change
- The prognosis is generally poor for such malignant tumors
- They can occur at any age
- More common during reproductive years (16-55)
- Peak incidence from 20-40
- During adolescence, 50% of adnexal neoplasms are mature cystic teratomas
Locations
- Ovary, most commonly
- Bilateral from 8-25 % of the time
- Teratomas may also occur in the
- Mediastinum
- Retroperitoneum
- Cervical region
- Brain
Clinical findings
- Most frequently found incidentally during physical or radiographic examinations for other reasons
- Symptoms, when present, include
- Abdominal pain, usually constant and low-grade
- Mass
- Abnormal uterine bleeding
- Back pain
- Bladder and GI symptoms
- Urinary frequency and change of bowel habits
Imaging Findings
- Conventional radiography
- Relatively insensitive, a conventional radiograph of the pelvis may identify
- A soft tissue mass, if large enough
- A fat-containing mass of lower density than the
surrounding soft tissue, a finding which is diagnostic
- Characteristic calcifications, such as
- “Popcorn” calcifications in uterine fibroids
- Rim-like calcifications in ovarian cystic lesions or
sometimes uterine fibroids
- A tooth or other bone (e.g. clavicle)
- Ultrasound
- Is the study of choice, either transabdominal or transvaginal
- US has been reported to have a 98% positive predictive value
for dermoids of the ovary
- Complex mass with echogenic components
- Mass itself is frequently echogenic producing “dirty acoustic shadowing”
- May occasionally be purely cystic (9-15%) or purely solid (10-31%)
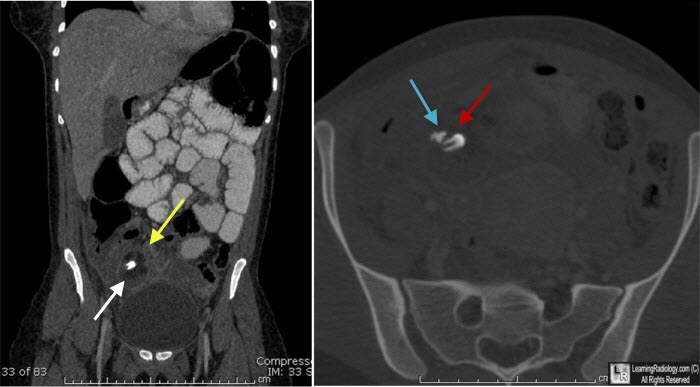
- CT
- MRI
- Hyperintense fat on T1 within fluid of low signal intensity
- Hyperintense mass on T2
Treatment
- Surgical removal can be accomplished with removal of the cyst
- Spillage of the contents of the cyst is associated with increased risk of chemical peritonitis
Complications
- Torsion is most common
- The larger the tumor, the more likely the risk of torsion
- Usually produces acute and severe pain
- Rupture
- Infection
- Autoimmune hemolytic anemia
Differential Diagnosis
- Benign or malignant ovarian neoplasm
- Endometrioma
- Tubo-ovarian abscess
- Pedunculated uterine fibroid
- Hydrosalpinx
- Ectopic pregnancy
- Pelvic kidney
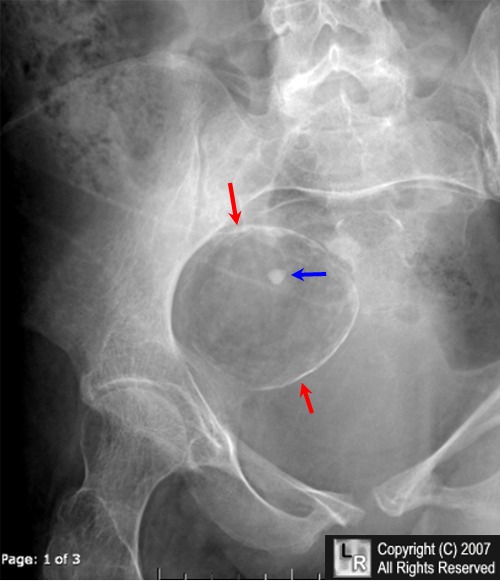
Dermoid cyst of the ovary. A close-up view of the right lower quadrant from a conventional radiograph
of the abdomen and pelvis shows a cystic mass with a rim-like calcification (red arrows) containing fat density lower than that of the surrounding soft tissue. There is a calcification within the mass (blue arrow) which represents a tooth. This is a diagnostic appearance for a dermoid cyst of the ovary.
For additional information about this disease, click on this icon if seen above.
For this same photo without the arrows, click here
Cystic Teratomas eMedicine Chad A Hamilton, MD, Edward Kost, MD, Margarett C Ellison, MD
|
|
|

){kind=link}
{kind=link}